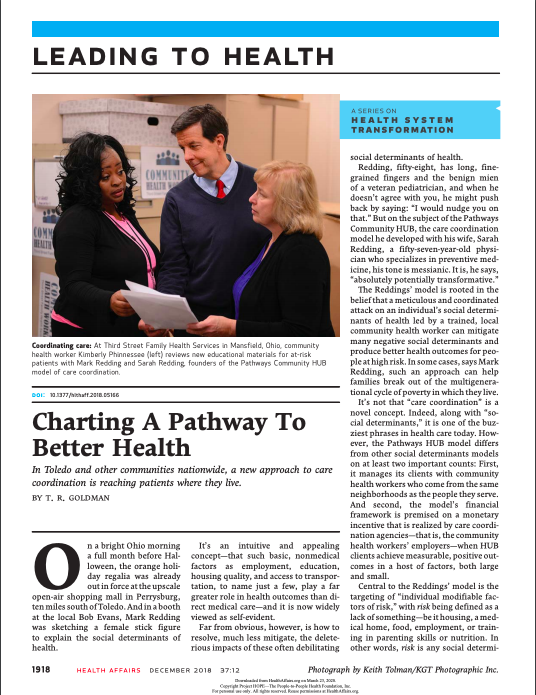
This article details how Toledo and other communities nationwide are implementing a new approach to care coordination to reach patients where they live, rooted in the belief that a meticulous and coordinated attack on an individual’s social determinants of health led by a trained, local community health worker can mitigate many negative social determinants and produce better health outcomes for people at high risk.
The Pathways HUB model differs from other social determinants models on at least two important counts:
- It manages its clients with community health workers who come from the same neighborhoods as the people they serve
- The model’s financial framework is premised on a monetary incentive that is realized by care coordination agencies—that is, the community health workers’ employers—when HUB clients achieve measurable, positive outcomes in a host of factors, both large and small.
There are twenty Pathways in the HUB model, ranging from housing to postpartum services and a behavioral health referral. There are broad Pathways such as social services, which includes twenty-five subcategories or tools such as a telephone, food stability, or a plan to start tackling medical debt. Each Pathway has an outcome, a specific metric that must be completed before the community health worker’s employer is paid—typically by the patient’s managed care plan or a government entity such as a local department of health.
This article is part of a series on transforming health systems published with support from the Robert Wood Johnson Foundation.